All forms of chronic kidney disease, once advanced enough, can cause fluid overload along with a number of electrolyte disturbances. In other words, these problems can be secondary to the CKD itself. Another type of kidney disorder, where the glomeruli leak significant amounts of protein into the urine, is called nephrotic syndrome. This process can cause severe fluid overload even when kidney function is otherwise normal. Many times, the first sign of a primary glomerular disease is edema or fluid overload, which is secondary to this process.
Disorders outside of the kidney are commonly the root cause of fluid overload. Cardiovascular dysfunction, where the kidneys receive reduced blood flow, is one such disorder. Severe liver disease can also cause shunting of blood away from the kidneys and result in fluid retention and overload. Finally, endocrine disorders such as hyperaldosteronism can also be the root cause of fluid overload.
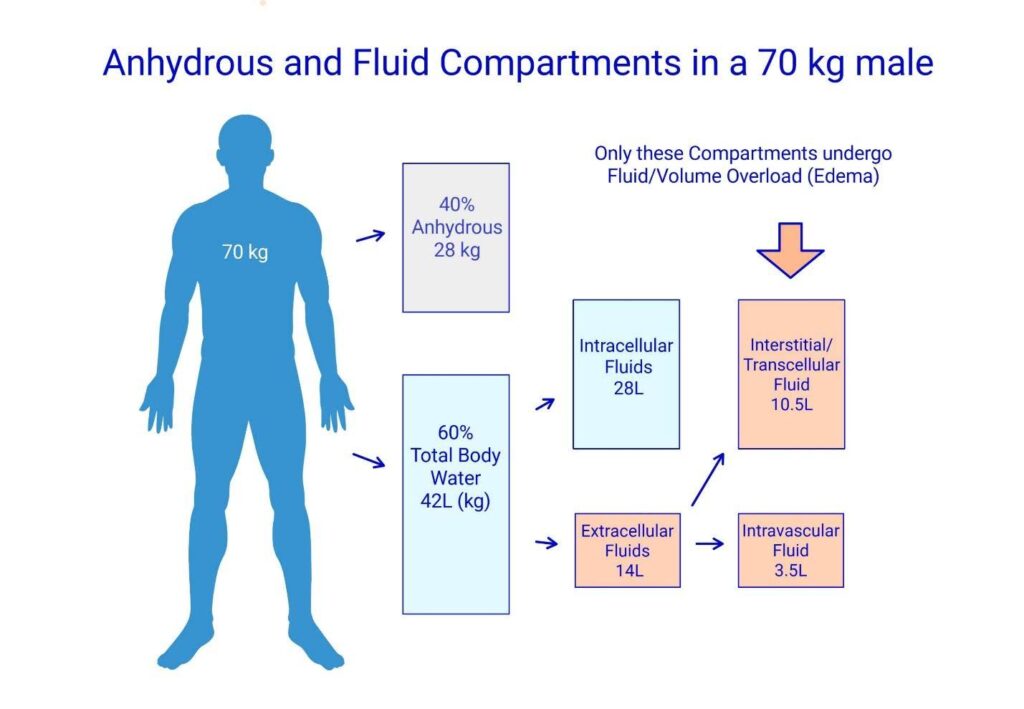
As a brief background, fluid overload can be more accurately described as extracellular volume overload. This fluid is kept in the extracellular space in a form of an isotonic sodium solution, with the primary anions being chloride and to a lesser degree, bicarbonate. Regardless of the root cause, the final common pathway for fluid overload is reduced excretion of sodium salts and water by the kidneys.
Aside from chronic kidney disease some genetically based disorders of ion channels/transporters can cause severe electrolyte derangements, particularly of potassium and magnesium. Gastrointestinal disorders such as chronic/recurrent diarrhea or vomiting, as well as malabsorption can cause electrolyte abnormalities. Endocrine disorders and prescription drug side effects can also be the root cause for electrolyte disturbances. Additionally, eating disorders and alcohol abuse often cause disordered electrolytes.

